

Background: Acquired thrombotic thrombocytopenic purpura (aTTP) is a rare and life-threatening hematologic disorder. The decision to start plasma exchange is challenging in clinical practice, due to aTTP rarity, and the extensive differential diagnosis with other thrombotic microangiopathies (TMA). Although the ADAMTS13 activity measurement is essential to aTTP diagnosis, a rapid quantification is unavailable in most centers, being necessary to develop clinical prediction models to evaluate severe enzymatic deficiency. The first model developed was Bentley score, followed by French score and more recently PLASMIC score. Studies comparing these 3 methods are scarce. The criteria of published scoring models are summarized in Table1
Aim: To compare and evaluate the discriminative power of the Bentley, French and PLASMIC scores in predicting severe ADAMTS13 deficiency (≤10%) in our group of patients (pts).
Methods: We performed a retrospective analysis of pts with ADAMTS13 activity tested between 2008 and 2019, in a single center. Pts were divided in two groups: ADAMTS13 activity ≤10% (ADAMTS13≤10%) and >10% (ADAMTS13>10%) and then stratified according to the 3 scores. We evaluate sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) to predict low ADAMTS13 activity. Diagnostic accuracy was tested using the area under the ROC curve. A P-value of <0.05 was considered statistically significant.
Results: ADAMTS13 activity was evaluated in 119 pts with suspected aTTP. There was a female predominance (60.5%; n=72) and the mean age was 54±20 years. Thirty-one pts had ADAMTS13≤10% and 27 (87.1%) of them had been diagnosed with aTTP, two were inherited thrombotic thrombocytopenic purpura and the other two were sepsis associated TMA. Comparing the groups ADAMTS13≤10% and ADAMTS13>10%, pts in the first were younger (46±18 vs 57±21 years; p=0.008), had lower platelet count (23.04±27.1 vs 47.79±37.6x109/L; p<0.001), and lower creatinine value (1.25±0.8 vs 2.92±4.2 mg/dL; p<0.017). ADAMTS13≤10% group had a higher reticulocyte count (5.99±5.0 vs 3.46±3.4%; p=0.005) and higher indirect bilirubin levels (2.59±2.1 vs 1.59±2.2 mg/dL; p=0.013). There were no statistical differences in hemoglobin, MCV, INR, D-Dimers and antinuclear antibodies (ANA's) positivity among the two groups.
PLASMIC score was calculated in all pts. Due to missing data, Bentley score was only applied in 44.5% (n=53) and French score in 54.6% (n= 65) pts.
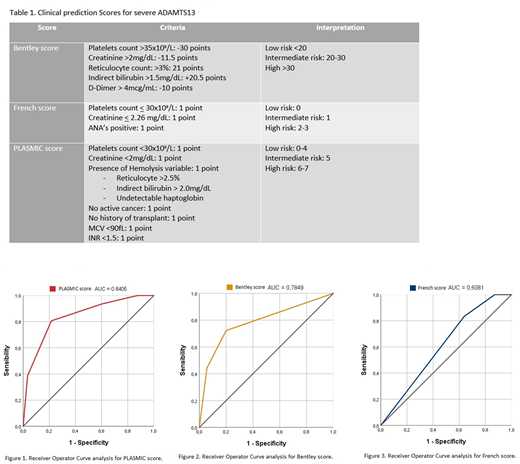
Using a high-risk PLASMIC score as the predictor, the sensitivity was 80.6%, specificity 78.4%, PPV 56.8% and NPV 92.0%. The C-statistics for high PLASMIC score cut-offs (>5 points) was 0.80 (95% confidence interval [CI] 0.70-0.89) (fig.1).
Applying high-risk Bentley score vs low-to-intermediate-risk score, the sensitivity was 44.4%, specificity 94.3%, PPV 80.0% and NPV 76.7%. The C-statistics was 0.69 (95% CI 0.53-0.86) using the high Bentley score cut-offs (fig.2).
The French score had higher sensitivity (83.3%), but lower specificity (36.2%), with 33.3% of PPV and 85.0% of NPV. Using the high French score cut-offs, the C-statistics was 0.60 (95% CI 0.45-0.75) (fig.3).
There were not statistically significant differences between PLASMIC and Bentley scores in the ability to predict low ADAMTS13 activity, and both performed better than French score (p<0.001; p=0.02, respectively).
Conclusion: In our cohort, the PLASMIC score showed to be the most balanced and efficient clinical prediction score, with high sensitivity and specificity. Bentley score was also a good predictor of ADAMTS13 activity, but had lower sensitivity and less applicability; French score was comparatively inferior.
Pts with low PLASMIC score are highly unlikely to have ADAMTS13 deficiency. PLASMIC score is easy to calculate and readily usable in most emergency settings while the French and Bentley scores require additional laboratory data, which is not always accessible.
These results support the previously published data, showing PLASMIC score as a helpful complementary tool in clinical practice recognizing high-risk pts when ADAMTS13 activity measurement is not available.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal